Signal acquisition
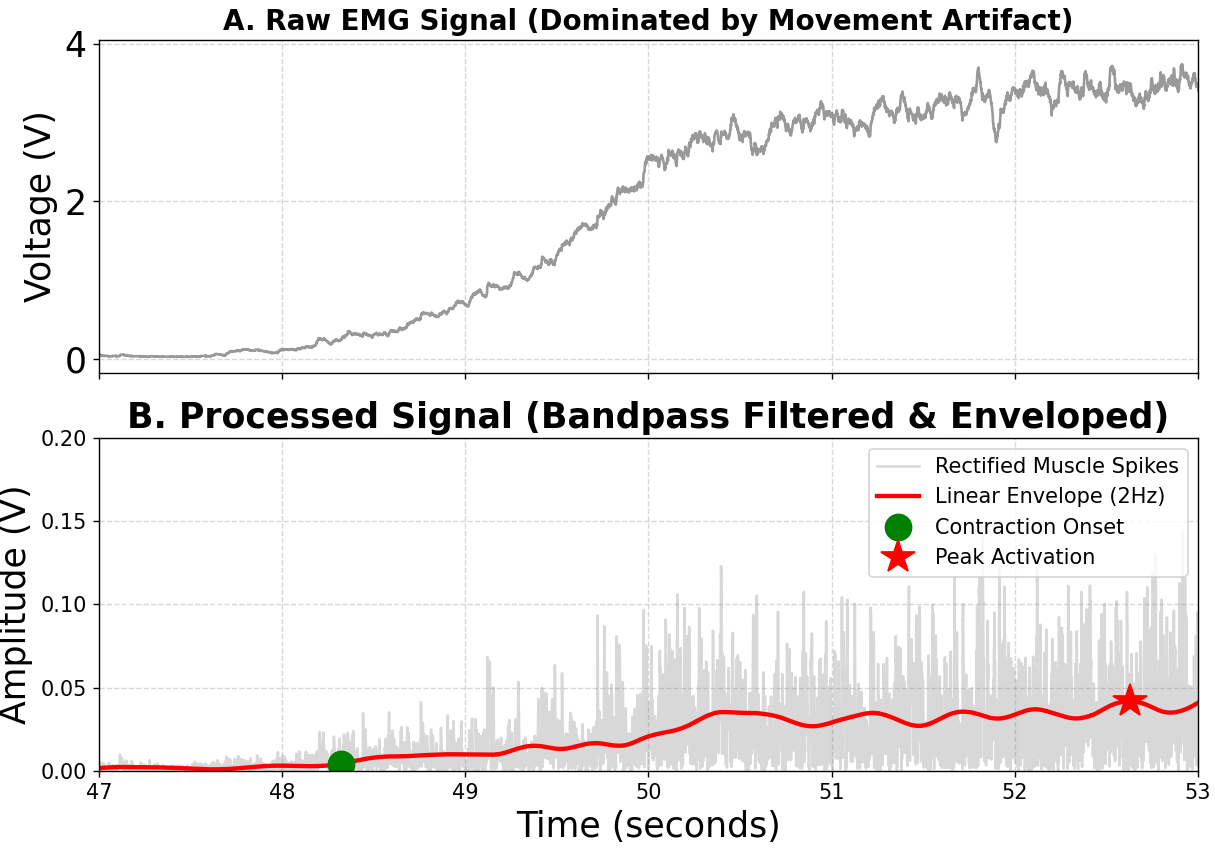
EEG was captured with the OpenBCI Ultracortex Mark IV headset and EMG was recorded through a MyoWare 2.0 sensor setup, creating a pilot pipeline for right-arm movement analysis.

Anvay Sheth, Paarth Karandikar, Thomas Healey, William BarrettProject Students

Dr Justin GallagherSupervisor
The project group developed a proof-of-concept control framework for home-based upper-limb rehabilitation. The project investigated whether non-invasive brain and muscle signals could be acquired, processed, classified, and translated into a usable assistance signal for the MyPAM rehabilitation robot.
The work brought together EEG abnormality detection, EMG-based stroke assessment, biomechanical validation, and a proposed closed-loop control strategy. Its central aim was to move rehabilitation support toward a more personalised, data-driven process in which assistance can adapt to the user's neurological state, movement intent, and muscle activation.
The project connected sensing hardware with an assistive rehabilitation device. The Ultracortex Mark IV headset supplied EEG data for estimating neurological activity, while the MyPAM robot represented the platform that could use those insights to adapt upper-limb assistance.
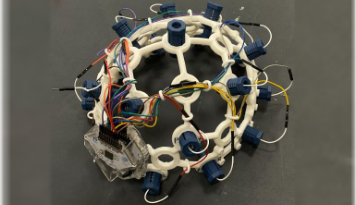
The 16-channel OpenBCI Ultracortex Mark IV was used as the non-invasive EEG acquisition platform. Its role was to capture cortical activity linked to neurological state and movement intent, giving the control system a brain-signal input that could contribute to an adaptive assistance score.
MyPAM provided the rehabilitation context for the project. The proposed control framework was designed so EEG and EMG-derived scores could inform how much support the robot should provide, helping translate physiological assessment into responsive upper-limb therapy.
The project is structured around five connected workstreams, each contributing a specific signal, validation method, or control decision to the wider MyPAM concept.
EEG was captured with the OpenBCI Ultracortex Mark IV headset and EMG was recorded through a MyoWare 2.0 sensor setup, creating a pilot pipeline for right-arm movement analysis.
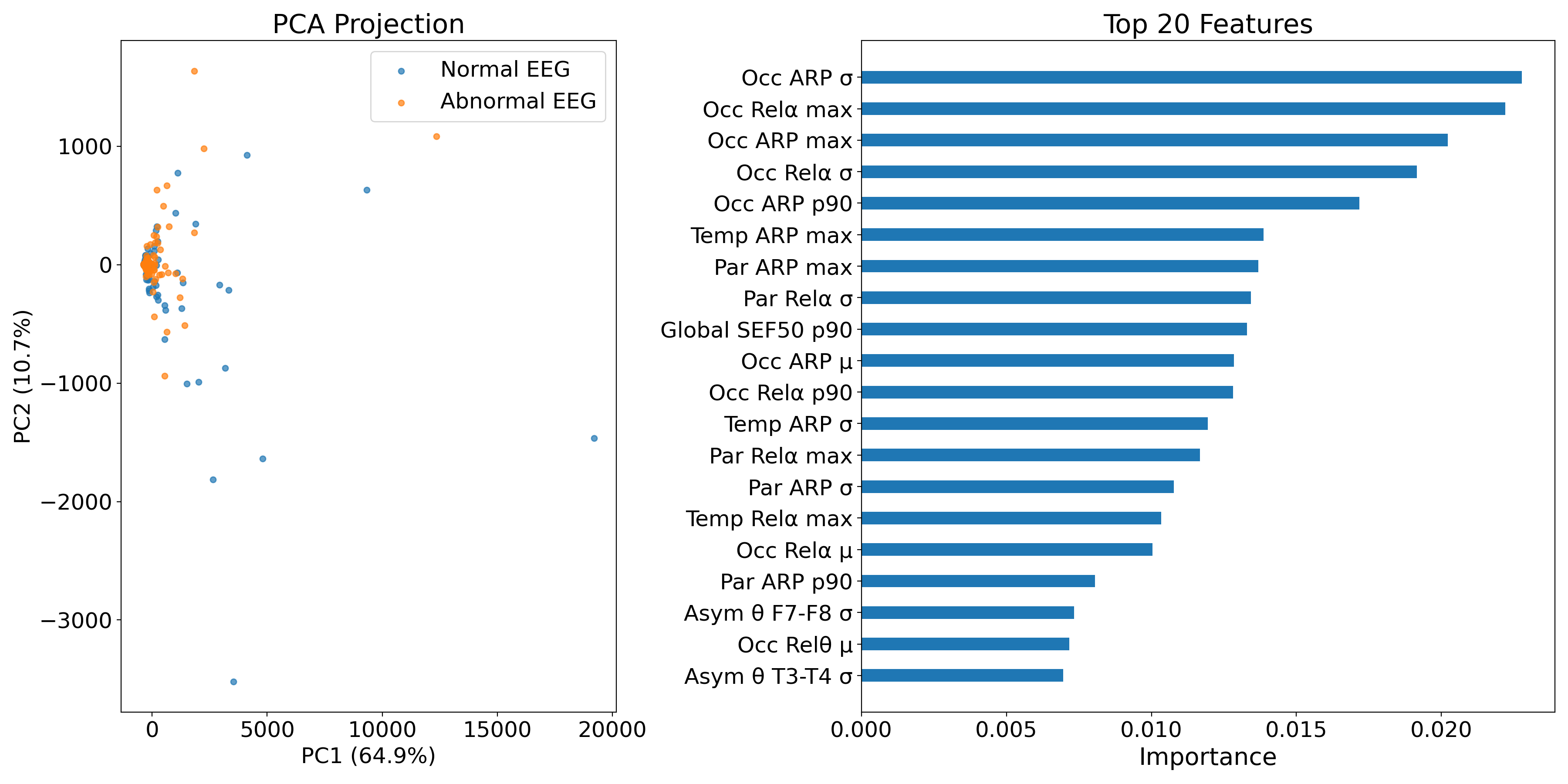
A Random Forest model used frequency, time, and spatial EEG features to estimate neurological abnormality and convert it into a continuous assistance-relevant score.
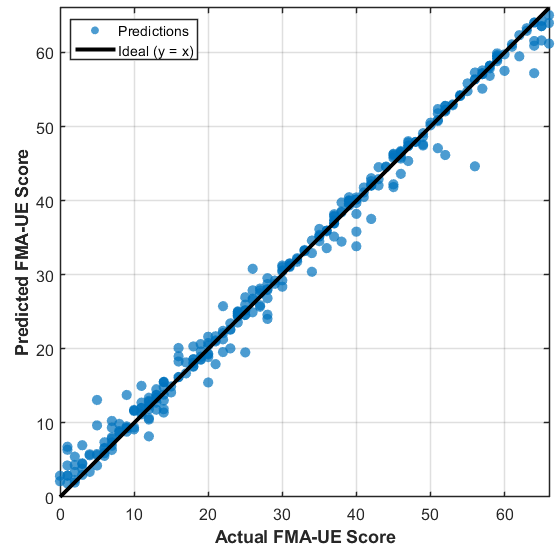
The EMG pipeline extracted muscular activation features, compared classifier performance, and explored continuous severity estimation aligned to the FMA-UE scale.
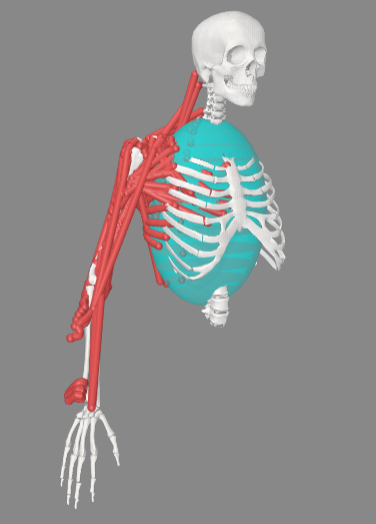
OpenSim was used to reconstruct upper-limb movement and compare modelled biceps activation against measured EMG trends.
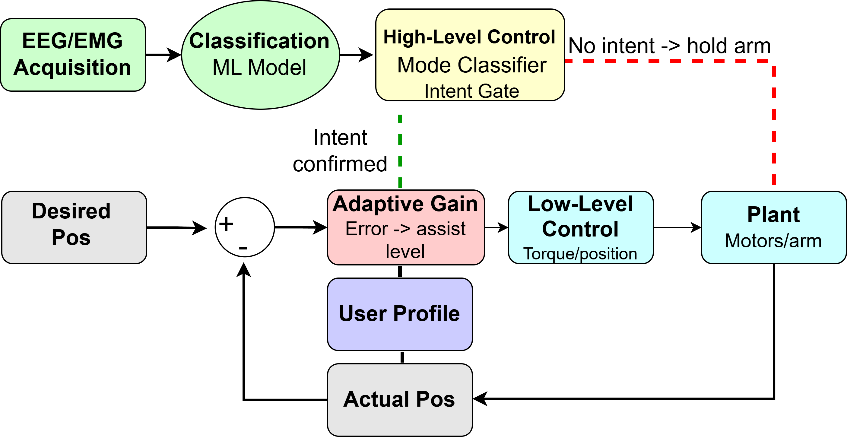
The final architecture proposed high-level intent gating, adaptive assistance gain, and low-level motor control for safer, more responsive MyPAM support.
EEG signals provided a neurological perspective by detecting cortical patterns linked to abnormality and movement-related activity. EMG added direct information about muscle recruitment and physical activation. Together, the two modalities created a stronger basis for adaptive assistance than either signal could provide alone.
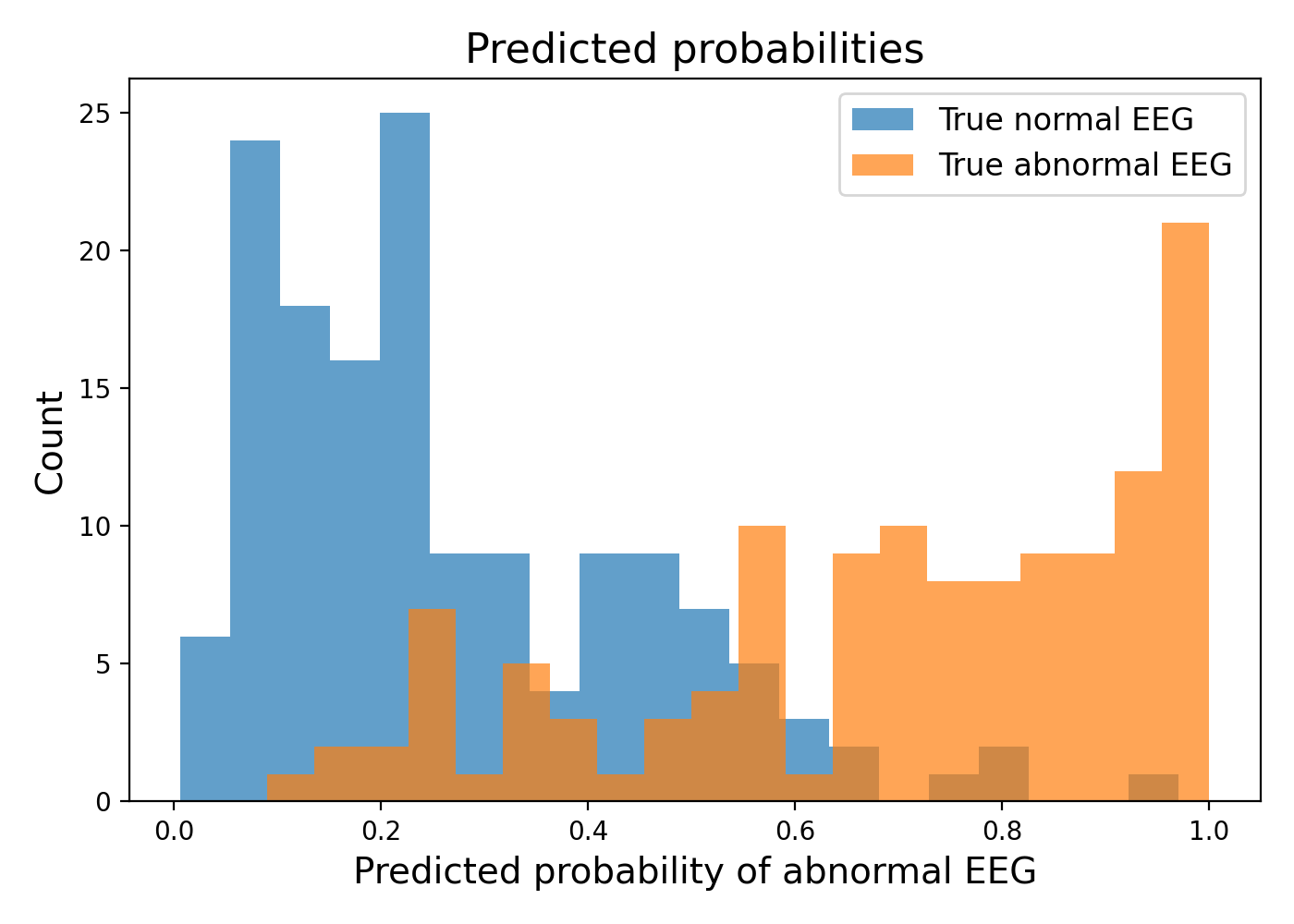
Normal versus abnormal EEG classification across 276 unseen recordings.
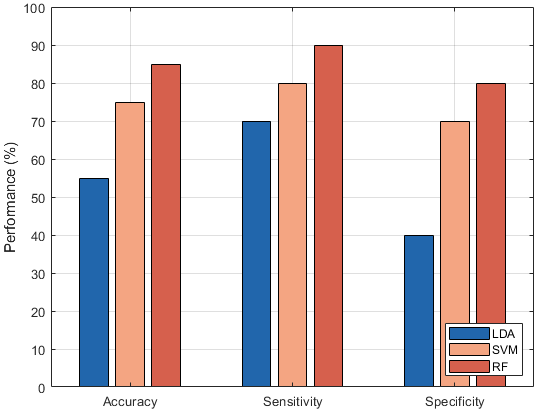
Comparable performance across normal and abnormal classes.
Strong separation across receiver operating and precision-recall analysis.
Random Forest performance under leave-one-subject-out validation.
Proof-of-concept severity estimation on synthetically generated data.
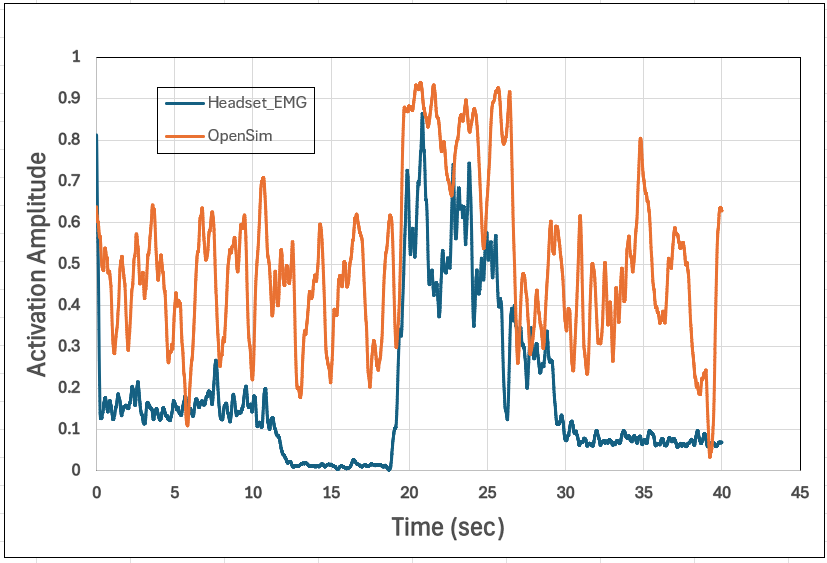
Difference between headset EMG and OpenSim activation peaks in one bicep curl test.
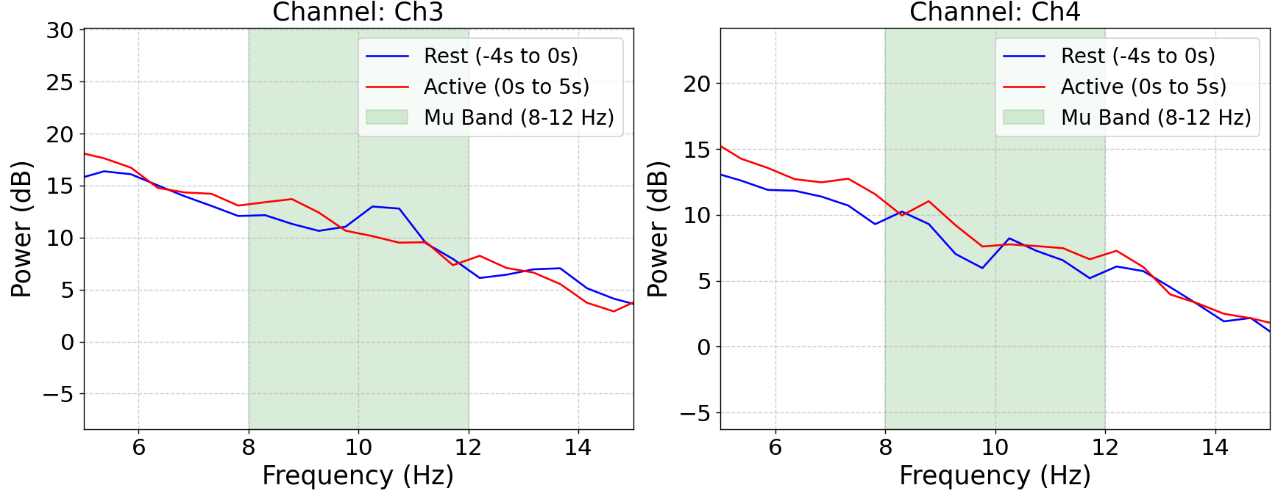
The EEG model was not treated as a diagnostic tool. Instead, its predicted probability of abnormality was interpreted as a relative signal that could contribute to adaptive assistance. Higher probability values indicate greater similarity to abnormal EEG patterns learned during training and could therefore map to higher support from the robot.
This approach is important because rehabilitation decisions are rarely binary. A continuous output allows MyPAM to respond more gradually, particularly when combined with EMG-derived muscle activation and movement information.
The validation work reconstructed upper-limb movements in OpenSim and used Static Optimisation to estimate biceps activation. The workflow compared those simulated trends with measured EMG from patient datasets and a headset-based bicep curl experiment.
Exact numerical matching was not expected because EMG measures electrical muscle activity while OpenSim estimates activation from a model. The useful finding was that the workflow captured comparable activation regions and timing trends, supporting its role as a validation layer for future MyPAM data.
The project demonstrated technical feasibility, but several components require further development before practical deployment. The EEG subtype classifier relied on synthetic data, the EMG severity model also used generated data, and the OpenSim workflow used generic modelling assumptions.
The project demonstrates how brain and muscle signals can be brought into a single rehabilitation control framework. By combining EEG-based abnormality scoring, EMG-based muscle assessment, biomechanical validation, and closed-loop assistance logic, it outlines a pathway toward more responsive home-based therapy.